Avalanche emergency : first aid for avalanche accidents
16.07.2025
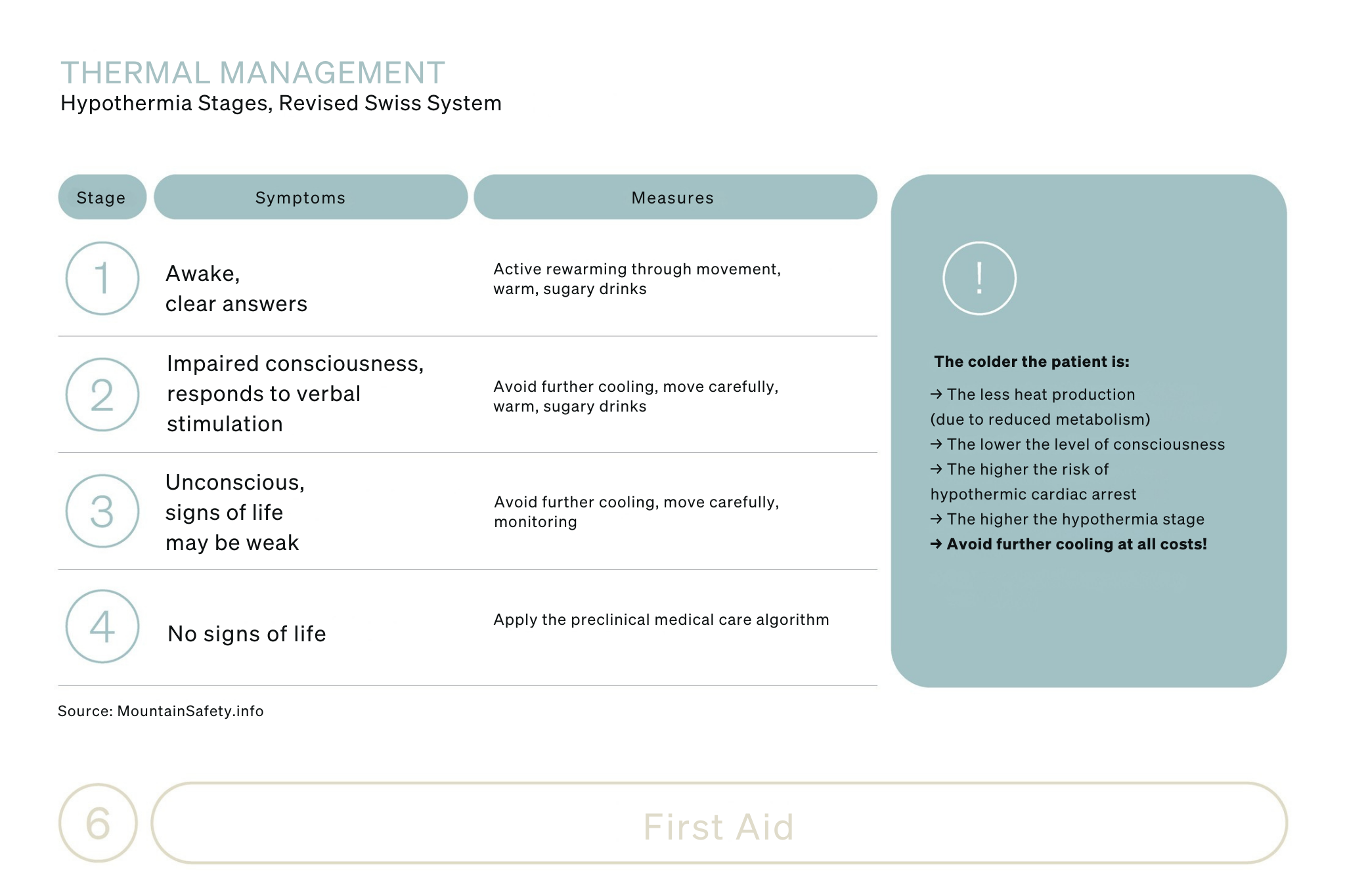
More than half of all people involved in avalanche incidents suffer no or only minor injuries. Around 32 percent of the people involved suffer serious injuries, while the fatality rate of people involved (regardless of burial depth) is around 13 percent. The prognosis for a buried person depends primarily on the degree of oxygen deprivation and/or the type of possible traumatic injury. In rare cases, hypothermia can also be fatal in the event of a long-term burial lasting more than 60 minutes.